E is for Ejection
- Ejection fraction
-
Rate qualitatively
- Normal - >50%
- Moderately depressed 30-50%
- Severely depressed <30%
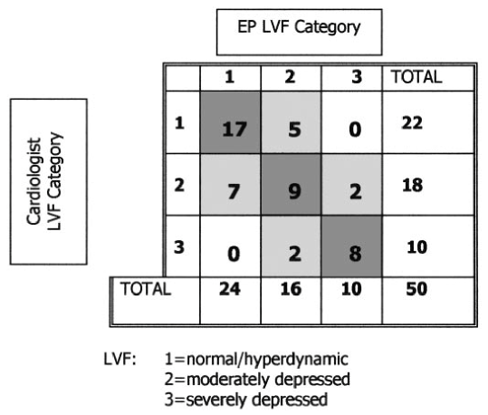
Moore et al. Acad Emerg Med 2002; 9:186-193.
Good
Bad
Narration
So the second E is E for Ejection, this is commonly known to be ejection fraction, which is the percentage of blood being ejected from the heart. Qualitatively measured, severely depressed when the EF is less than 30%. We were among the first investigators to study this - EP being compared to radiologists. So estimating the heart and being able to tell good from bad is the important part here. Here we see a dilated cardiomyopathy where we see less than 15% or less of blood being ejected from that cavity.
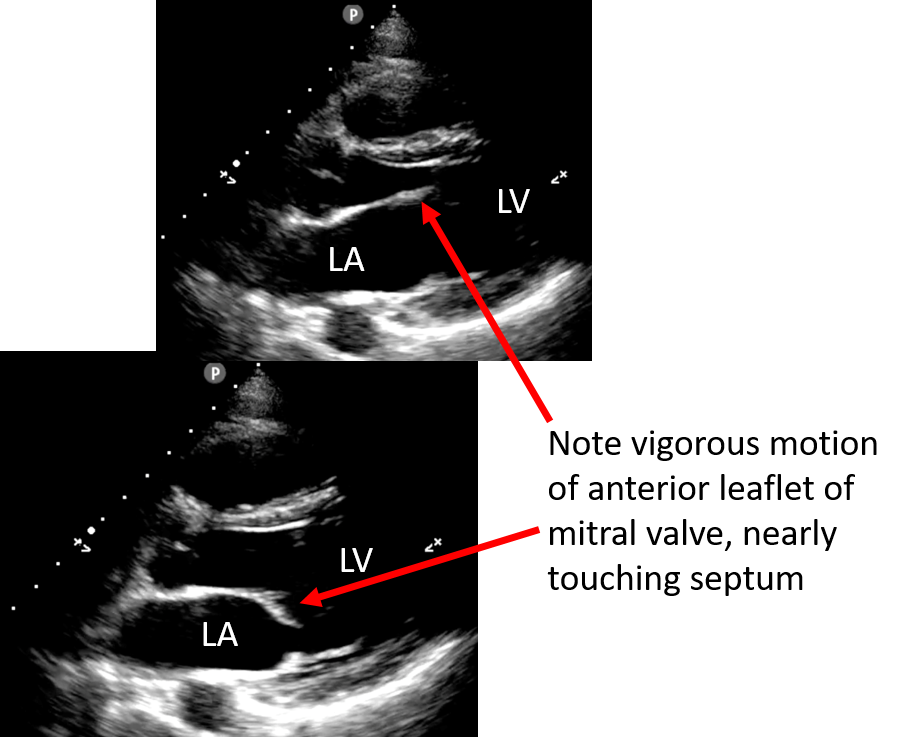
Parasternal long axis normal EF
Narration
A parasternal long axis view is a very good way to start looking at the ejection fraction. When we look at this view we see the right ventricle is very anterior and then the left ventricle with the mitral value, and in addition to keeping your eye on the endocardial borders and seeing how well they're squeezing a good thing to watch is that mitral valve, the anterior leaflet that is, which is vigorously moving and slapping up against the septum and this is a normal ejection fraction on a parasternal long axis view.
PSLA severely decreased EF
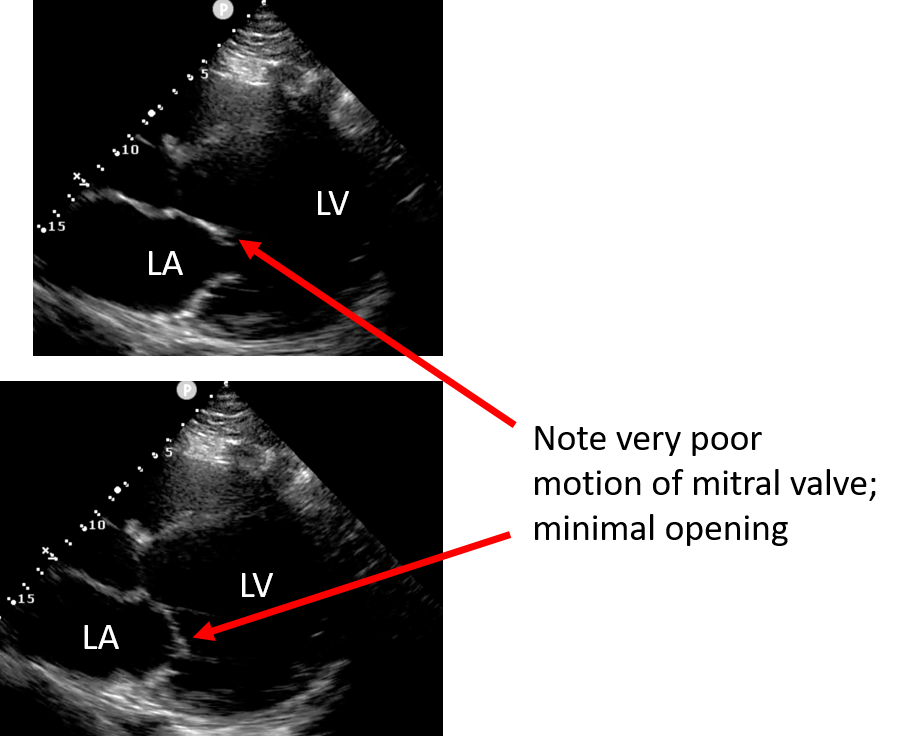
Narration
Here is a view that shows a very poor ejection fraction, again probably 15% or less. It's a very large, dilated left ventricle and a small percentage of blood is actually leaving that ventricle. If you watch that mitral valve carefully again, the anterior leaflet is opening, but only slightly – it’s not getting anywhere near the septum and this is a good clue that the ejection fraction is severely depressed.
- Parasternal short axis
- Papillary muscle/mitral valve level
Good EF
Bad EF
Narration
Another excellent view for estimating ejection fraction is the parasternal short axis, and you turn the probe counter clockwise 90 degrees and there's really sort of the 4 levels of the parasternal short axis, from apical to papillary muscle to mitral valve to aortic valve level. The best place to look is typically at the papillary muscle level. In the bottom left, we see a parasternal short axis view with good circumferential circular squeeze all the way around. You can see the papillary muscles in the inferior part of the field of view there. This is contrasted to the upper right pane where we see a clip of a parasternal short axis that is really not squeezing well at all, its ejecting probably well under 30% of the blood and you can see the difference between the squeeze in the circumferential view of the parasternal short axis.
Subxiphoid
Good EF
Bad EF
Narration
This view shows a subxyphoid view which we can also use to estimate how the left ventricle is doing. Again, on the bottom left pane we see the left ventricle in the far field squeezing quite well, this is as opposed to the right upper pane where the left ventricle is dilated, hypokinetic and again you can see that anterior leaflet of the mitral valve which is opening, but not briskly and certainly not touching the septum of the left ventricle. This is a poor ejection fraction again probably about 15% as opposed to a good ejection fraction well over 50% in the lower left.
Apical
Good EF
Poor EF
Narration
The apical view can certainly be used, and here again we see the difference between good and bad. The lower left pane shows the left ventricle on the right side of the screen as it is viewed contracting well, and this is contrasted to the upper right pane where you can see a somewhat dilated left ventricle that’s really not squeezing with poor motion of the mitral valve leaflets. Of note, the upper right pane also does show a small to moderate pericardial effusion seen just behind the right atrium.
- Moderate EF – 30-50%
- More difficult to call
PSAX
PSLA
Narration
So we're really trying to differentiate good from bad or a really poor or depressed ejection fraction from normal. The one that's a little more difficult to call is when its moderate, and this is typically considered to be in the range of about 30-50%, and these are two examples of moderate ejection fraction I'd probably put it in the 40% range, maybe a little lower. In this case it’s not quite as bad as the ones we've seen, but also certainly not normal and you can see that in both the parasternal short axis view with the papillary muscles in the lower left and the parasternal long axis view. Notice in the upper right hand pane that the mitral valve is moving more vigorously then some of the ones that we saw, but is not getting close the septum as it would in a completely normal ejection fraction.
This website provides professional medical education. For medical care contact your doctor. 2024 ©MedEdu LLC. All Rights Reserved. Terms & Conditions | About Us | Privacy | Email Us | 1 | n 1