Peripheral Vascular Access
Learning US Guided Procedures
Narration
So if you want to learn how to do ultrasound guided procedures, I'd recommend you start with peripheral venous access. These tend to be small vessels, and if you can access these well, then other procedures become easy. In fact, the clip on the right here shows IJ access, it’s a pretty large vessel and that's actually quite simple once you can access the much smaller peripheral veins. I would estimate it takes about 30 peripheral IVs using US guidance to get really good at it and would recommend that you try to use the single person dynamic guidance where you're actually watching the tip of the needle go into that vessel in real time.
Peripheral IVs
Narration
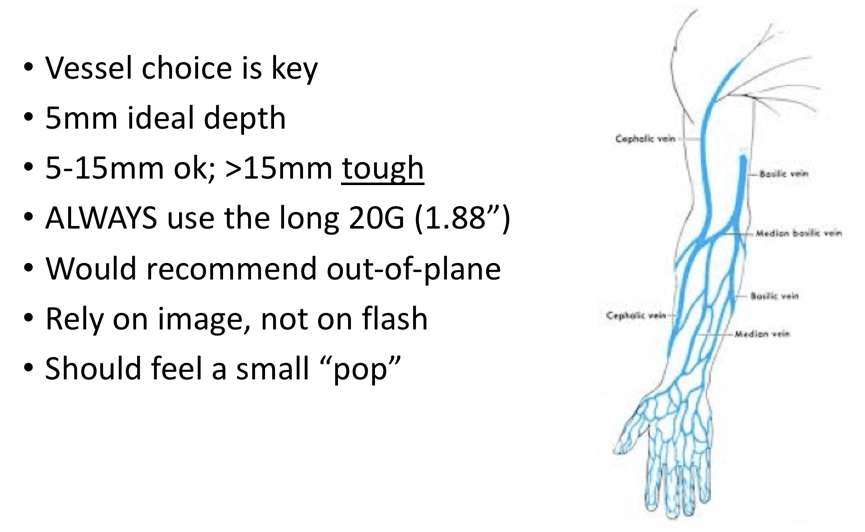
This shows a map of the arm, the basilic vein is on the medial side of the arm often 5-10mm deep. You can also do the antecubital or various veins in the forearm; and as far as depth, 5mm is ideal for ultrasound guidance, less than that you can often do it without ultrasound, ultrasound may actually get in the way. 5-15mm is pretty good, once it gets over 15mm it is pretty tough. I would recommend you always try using the longer catheters - often the 1.88 inch ones are ones we use, they also have even 2.5 inch catheters. As mentioned before, when I do my vascular access I use the out-of-plane approach where I put that needle over the middle of the vessel land track it going into the middle of the vessel, I tend to rely on the image, not on the flash. The flash can be deceiving - you can back wall the vessel and get a flash, you should feel a small pop, but really you want to see that vanishing target sign when you have the tip of the needle in the center of the vessel.
Why Am I Not In?
Narration
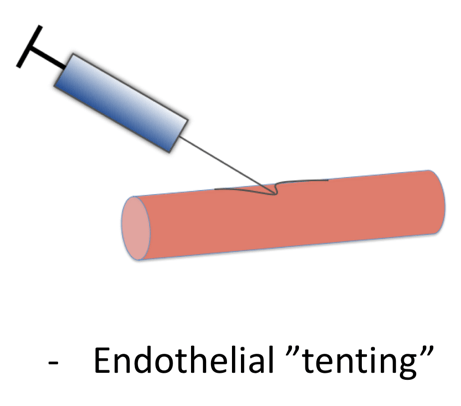
So what makes this tough and why are you not in sometimes? This is showing an in-plane or long axis approach to the vessel with the shaft of the needle and the tip and you can see how the endothelium or the covering of that vessel is kind of tenting in before the needle actually pops in and this can make it tough sometimes to make sure that you're inside a peripheral vessel.
Why Am I Not In?
Narration
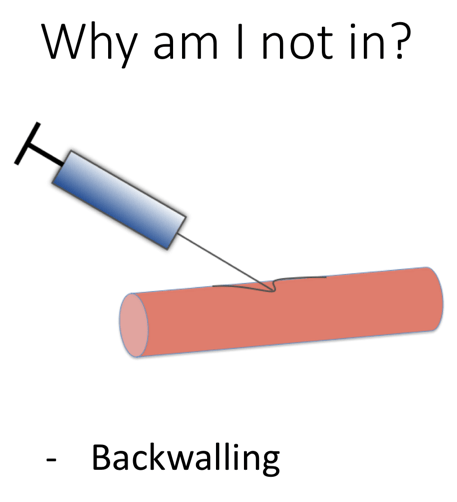
The other thing that can happen is because these vessels are small and they collapse easily is that the needle can push the walls together and as soon as you penetrate one wall you go right through the other. This called backwalling, and in this case you get behind the vessel and you can't thread it, so what you need to do is back the needle out slightly until the vessel opens and you can see the tip in the center of the lumen.
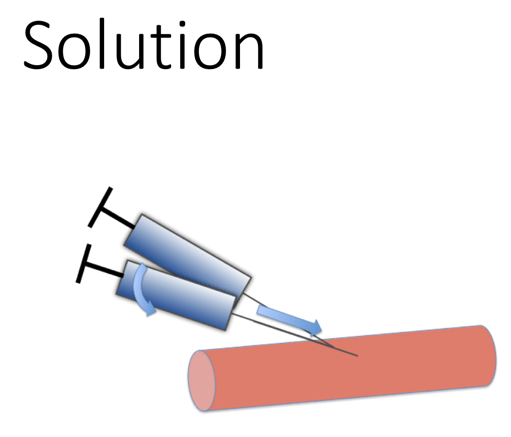
Solution
Narration
First of all, when you get in, try to flatten out that needle and advance it so that you see the tip in the center and again you see that target sign on the lower right image here- you want to fan distally to make sure that target vanishes or diapers to that the tip of the needle is terminating in the vessel.
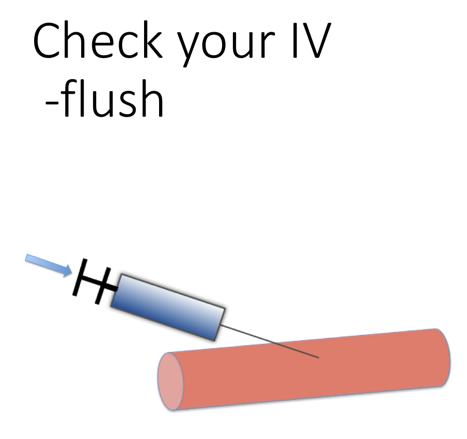
Check Your IV - Flush
Narration
Once you've placed your catheter you can leave it in there and check it with a flush, take a little saline, maybe agitate it with some air, eject the air and inject the saline to see the flush within the vessel.
pv: 1
This website provides professional medical education. For medical care contact your doctor. 2024 ©MedEdu LLC. All Rights Reserved. Terms & Conditions | About Us | Privacy | Email Us | 1 | n 1